Design Artifact
Step 4 — Performance support card.
The companion Canva performance support card is a 4×6 laminate-style card designed for two use cases: a physical card kept at a workstation, and a digital PNG pinned in a team communication channel.
It contains exactly three things — and deliberately nothing else:
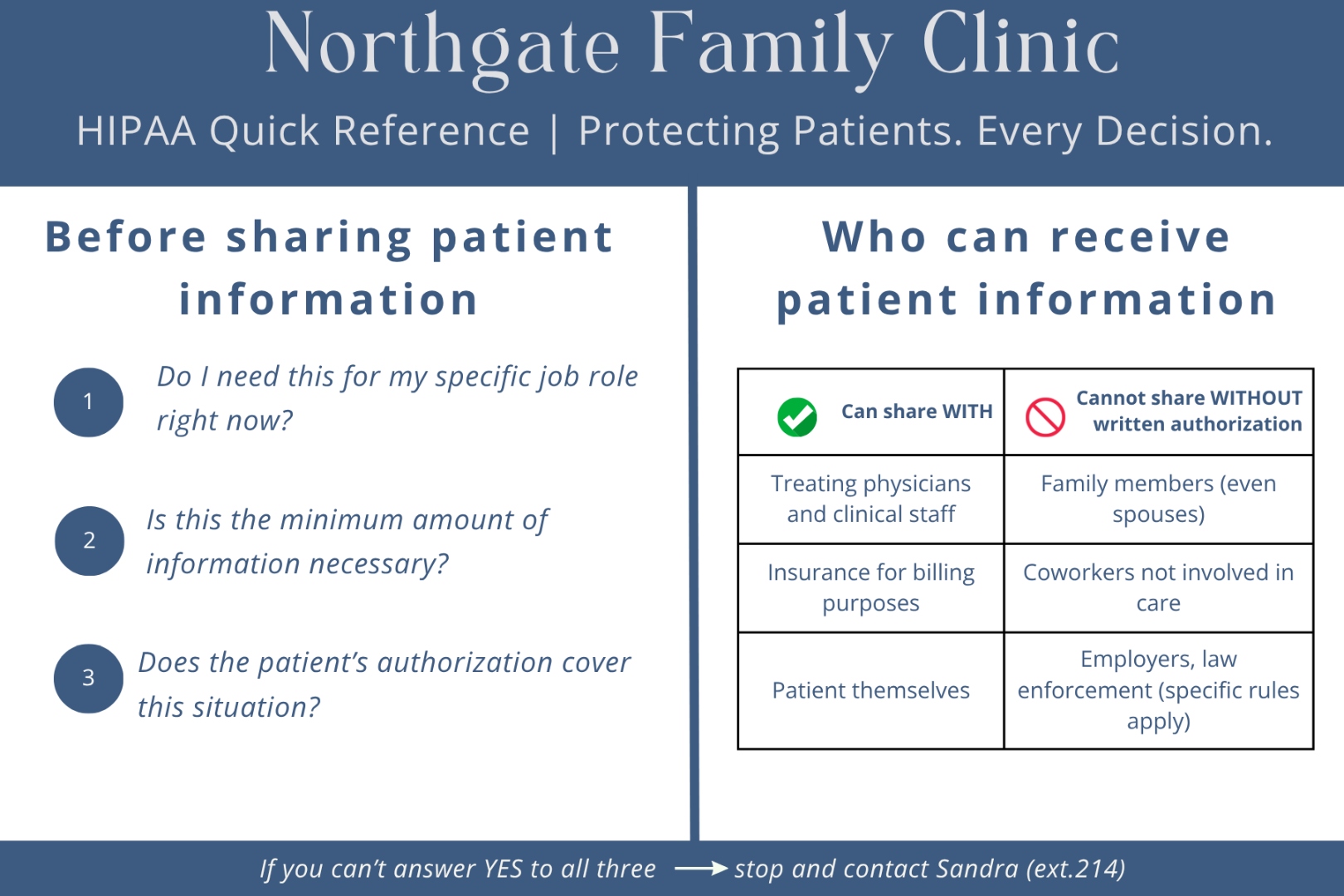
1. 3-Question Compliance Check
Three yes/no questions that function as a decision gate before any patient information is shared.
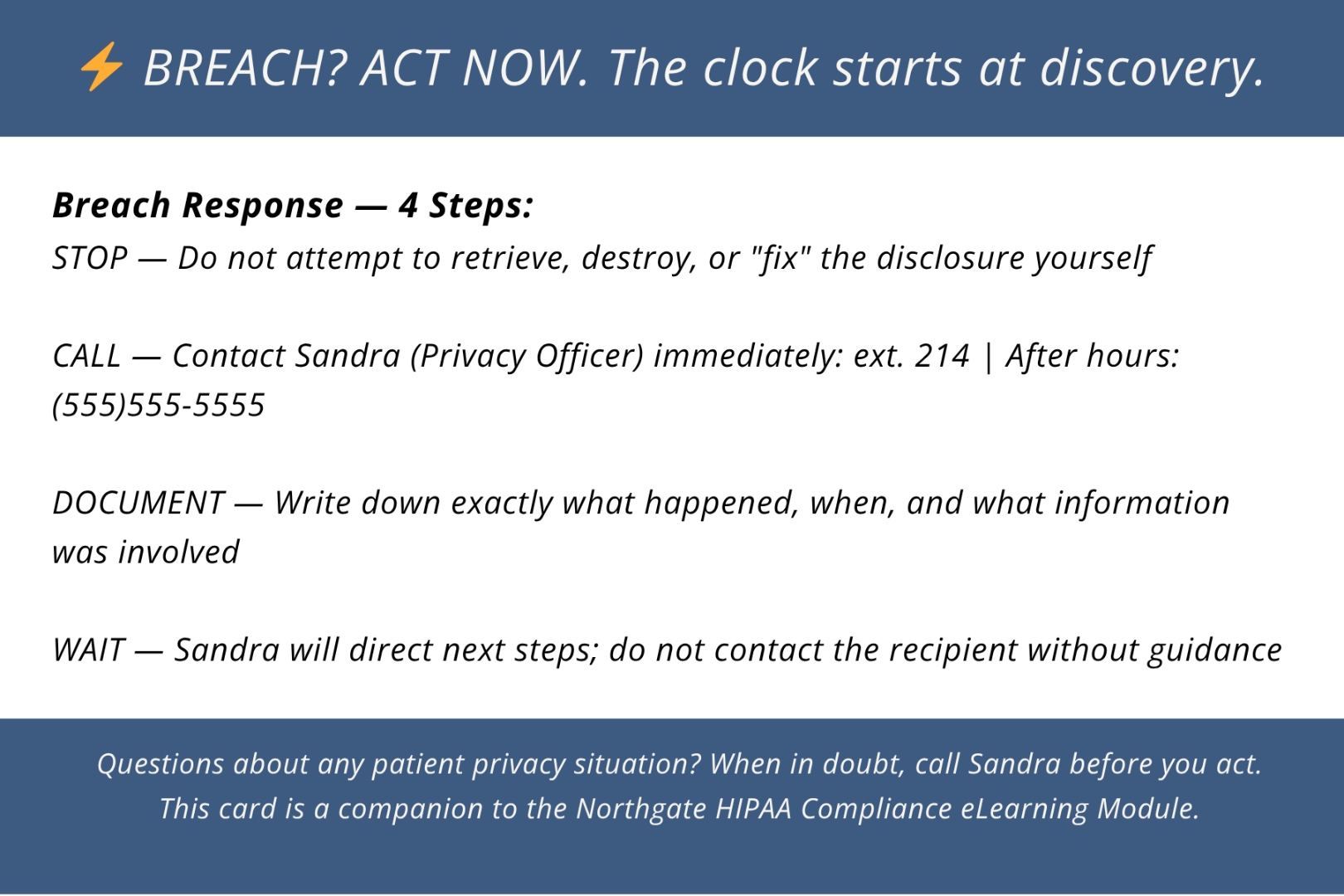
2. Breach Response Sequence
Four steps to take in the first minutes after a potential disclosure, including the Privacy Officer's direct extension.
3. Clear Escalation Signal
"When in doubt, call Sandra before you act" — naming the specific person and the specific moment to call.
The card deliberately does not reproduce HIPAA rules or regulation summaries. It is not a reference document — it is a decision tool. The moment of need is not the moment to read. It is the moment to act.